Since their introduction, vaccines have served as a cornerstone of public health in the United States and abroad. Vaccinating large numbers of people, especially children, has proven to be one of the most cost-effective options for enhancing and preserving life.
But the vaccine industry itself is at high risk for failure, with shortages becoming more and more frequent. For example, of the 12 pediatric vaccines recommended for all children, there have been severe shortages of more than half, ranging from a shortage of MMR-vaccine (measles, mumps and rubella) lasting seven months to a shortage of PNU-vaccine (pneumococcal infections like meningitis) lasting nearly two years! Immunizations for some children were delayed until adequate supply levels were restored. Inevitably, some children never "caught up" after supply levels were finally restored, remaining unvaccinated.
What has led to this fragile supply within the vaccine industry? It is a combination of challenging economic conditions for manufacturers and actions by the federal government which have distorted the market. 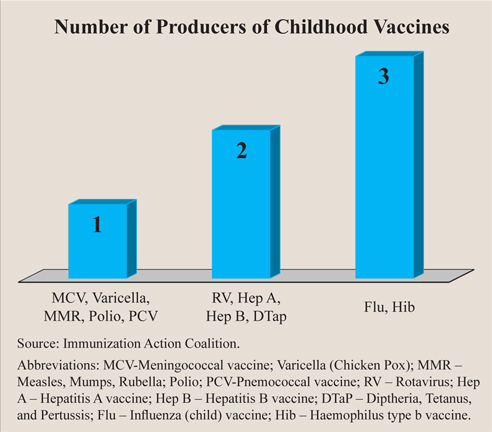
Problem: High Production Costs. About 60 percent of total production costs in manufacturing vaccines are fixed, meaning that those costs are incurred for any level of production and do not depend on the quantity produced. These fixed costs are also sunk costs, meaning they cannot be recovered. If a firm had to shut down production, these costs could not be recouped.
Production of the flu vaccine illustrates this troubling condition. In order for their vaccine to be effective, flu vaccine manufacturers have to predict nearly a year before the target flu season which strains of the flu virus will be prevalent and which strains they will immunize against. If their prediction is incorrect, the manufacturers can only cut their losses. In addition, if the flu season turns out to be mild, producers risk having large unsold inventories without the ability to decrease production costs. When sunk fixed costs are about 60 percent of total costs, this loss can be devastating to a manufacturer. With the average cost to bring a vaccine to market at about $700 million, sunk fixed costs can be so prohibitive that producers leave the vaccine marketplace.
Problem: Low Market Prices. The federal government is a heavy participant in the market for vaccines, creating substantial market distortions. In fact, it is a monopsony buyer, which is when a single buyer purchases the majority of a good produced. The federal government's position as a major buyer in the vaccine market increased dramatically with the introduction of the Vaccines for Children Program (VFC) in 1994. In 2002, VFC purchases alone were 41 percent of the entire vaccine market, with another 16 percent of purchases controlled by the Centers for Disease Control and Prevention (CDC) and a multitude of state and local agencies. In 2004, the VFC program alone accounted for $1.2 billion in sales. This gives the federal government tremendous leverage, or market power, allowing it to demand and receive below-market prices from manufacturers. The federal government can often negotiate a discount of 25 percent to 65 percent off the average wholesale price of a vaccine. For example, the catalog price of a single MMR dose in 2005 was $40.37. The CDC's negotiated price for the same dose was $16.67. In addition, state and local governments can purchase vaccines at the government-negotiated price.
Problem: Overregulation. The production of vaccines is under the jurisdiction of the Food and Drug Administration (FDA), whose regulatory oversight can cause shortages of important vaccines. In 1999, the FDA mandated the removal of thimerosal, a potentially toxic, mercury-based preservative used in vaccines. Despite warnings by the American Academy of Pediatrics and the U.S. Public Health Service that the danger posed by thimerosal was vastly outweighed by the danger of not vaccinating, the FDA proceeded to implement this requirement anyway. This action resulted in a 25 percent reduction in the already fragile supply of some childhood vaccinations like DTaP (diphtheria, tetanus and pertussis).
Result: Barriers to Entry. High fixed costs, low market prices and the influence of overregulation combine to produce prohibitive barriers to entry into the vaccine production market, which stifles competition and innovation. Thus, it is rare for new firms to enter the market and has also caused existing firms to exit the market. Further, vaccines are largely produced within individual nations due to differences in regulation. This means that companies do not produce vaccines for global consumption, which would allow for economies of scale and increase international competition. Due to these fragmented markets, domestic manufacturers incur higher production costs but face smaller potential markets. Due to the barriers to entry of new firms and factors encouraging existing firms to exit, the supply of childhood vaccines is fragile: There are just three manufacturers who supply any of the recommended childhood vaccines, and five of these vaccines are produced by only one firm [see the figure].
Result: Fewer Vaccinations. Manufacturers are going to direct capital to those products whose markets provide the most stability and highest profit margins. Vaccines account for only 2 percent of pharmaceutical revenues. Thus, if profit margins continue to decline, it is highly likely that pharmaceutical manufacturers will continue to replace vaccine production with more profitable drug production.
Conclusion. In effect, the federal government has the power to pressure firms into accepting below-market prices. But what the federal government cannot overcome are the negative secondary effects that result from artificially-low prices.
Low profit margins and artificially-low market prices have limited competition in the industry. The federal government should remove itself from the marketplace. The solution is less government interference, not more.
Matt Baumann is a research assistant with the National Center for Policy Analysis.
Abbreviations: MCV-Meningococcal vaccine; Varicella (Chicken Pox); MMR – Measles, Mumps, Rubella; Polio; PCV-Pnemococcal vaccine; RV – Rotavirus; Hep A – Hepatitis A vaccine; Hep B – Hepatitis B vaccine; DTaP – Diptheria, Tetanus, and Pertussis; Flu – Influenza (child) vaccine; Hib – Haemophilus type b vaccine.